Common types of dysgnathia
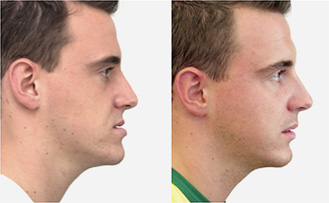
Underbite/overbite/facial asymmetry
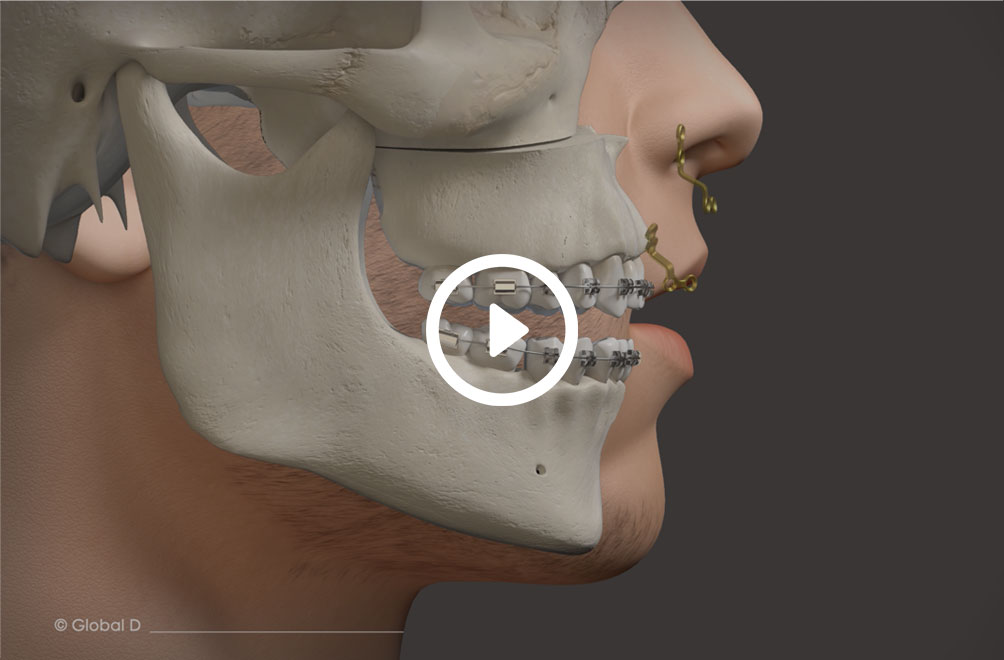
Repositioning the upper or lower jaw to create an optimal overbite and
profile normalization.
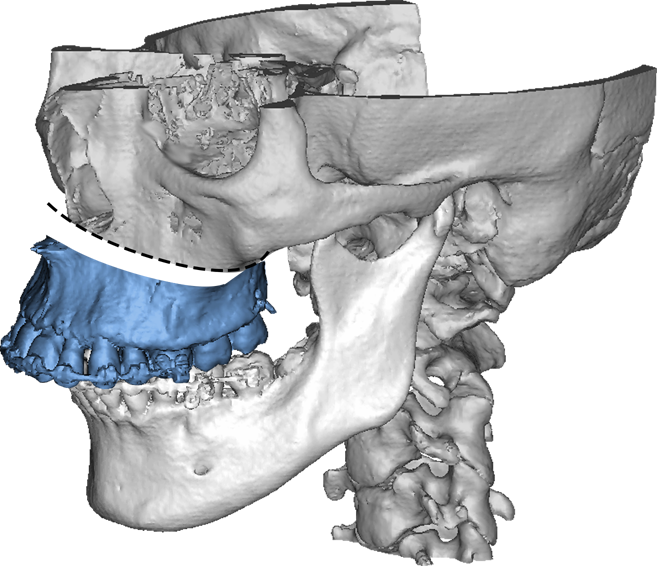
Combination of upper and lower jaw surgery (maxillomandibular realignment)
Underbite/overbite/facial asymmetry
facial asymmetries
Repositioning the upper or lower jaw to create an optimal overbite and
profile normalization.
Combination of upper and lower jaw surgery (maxillomandibular realignment)